Leg pain, numbness, or weakness radiating from your lower back? Here’s what may be behind it.
Most people have heard of sciatica. Fewer have heard the clinical term for what’s actually happening: lumbar radiculopathy. If pain starts in your lower back and travels down one leg, sometimes all the way to your foot, this is likely the condition your doctor is trying to rule in or out.
It’s more common than most people realize, and more treatable than most people fear. Understanding what it is and why it happens is a reasonable first step toward feeling less uncertain about where to go from here.
What Is Lumbar Radiculopathy?
Lumbar radiculopathy occurs when a nerve root in the lower spine becomes compressed, irritated, or inflamed. The lumbar spine sits between your ribcage and your pelvis, and it carries a significant amount of the body’s load through every movement you make.
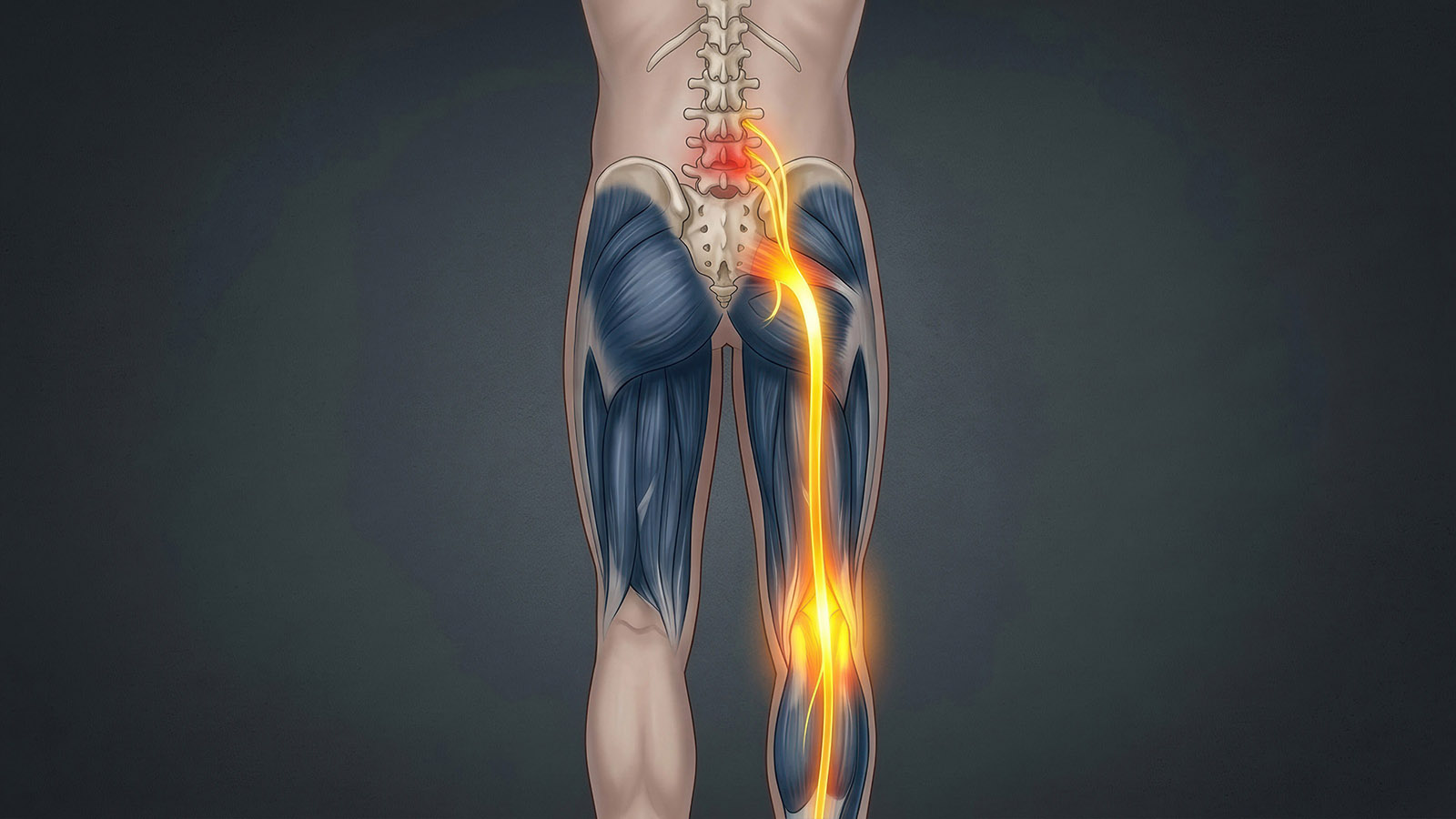
When a nerve root at this level faces pressure, it doesn’t just cause pain at the source. It sends signals along the entire path that the nerve travels, which is why you may feel pain, tingling, or numbness in your hip, thigh, calf, or foot rather than your back. That radiating quality is the hallmark of radiculopathy, and it’s what makes the condition feel so disorienting when it first appears.
Lumbosacral radiculopathy refers specifically to nerve involvement at the junction between the lumbar spine and the sacrum, the triangular bone at the base of your spine. This region includes some of the most commonly affected nerve levels seen in clinical practice.
Which Nerves Are Most Often Involved?
The lumbar spine has five vertebral levels, labeled L1 through L5, with the sacral segment below designated S1. The two levels most frequently associated with lumbar radiculopathy are L4-L5 and L5-S1.
L5 radiculopathy typically produces pain, weakness, or numbness along the outer hip, down through the leg, and into the top of the foot or big toe. Some patients notice difficulty lifting the front of the foot, a symptom called foot drop in more severe cases.
S1 radiculopathy tends to affect the back of the leg, the calf, and the outer edge of the foot. Many patients report weakness when pushing off the foot while walking, along with pain that worsens after standing for extended periods.
These patterns aren’t always perfectly predictable. Symptoms point in the right direction, but imaging and nerve testing confirm what’s actually happening and at which level.
What Causes Lumbar Radiculopathy?
A herniated disc is the most frequent cause. Think of the discs between your vertebrae as small cushions. When the soft inner material pushes through the tougher outer layer, it can press directly on a nearby nerve root. This happens most often at L4-L5 and L5-S1, where the spine absorbs the most load day to day.
Spinal stenosis is another common culprit, particularly in older patients. The canal through which your spinal nerves travel can narrow over time due to arthritis, bone spurs, or thickened ligaments. When that happens, the resulting pressure builds gradually, which is why stenosis-related radiculopathy often develops slowly rather than appearing overnight.
Other causes include degenerative disc disease, spondylolisthesis (where one vertebra slips forward over another), and, less commonly, tumors or infections near the spine. In some cases, more than one factor contributes at the same time, which is why a thorough evaluation looks at the full picture rather than stopping at the most obvious finding.
Recognizing the Symptoms
Lumbar radiculopathy feels different for different people, but most patients recognize some version of these experiences.
Pain is the most common complaint, typically described as sharp, burning, or electric. It usually travels from the lower back into the buttock and down one leg, and while it doesn’t always reach the foot, it often does.
Numbness and tingling frequently show up alongside the pain, sometimes in places that don’t seem obviously connected to the spine, like the toes or the sole of the foot.
Muscle weakness is less common but more important when it appears. If you’re noticing difficulty walking, instability on one leg, or the sense that a limb isn’t responding the way it should, bring that up with a physician sooner rather than later.
One thing worth knowing: imaging findings and symptoms don’t always match up the way you might expect. Some patients show significant compression on an MRI but feel relatively little pain. Others experience severe symptoms with findings that look modest on a scan. This is part of why a clinical evaluation matters as much as the imaging itself.
How Physicians Diagnose Lumbar Radiculopathy
Diagnosis begins with a detailed clinical evaluation. Your physician will ask about when symptoms started, what makes them better or worse, and whether you’ve noticed changes in strength or bladder and bowel function. A physical exam helps identify which nerve levels may be involved through reflex testing, muscle strength assessment, and mapping of any sensory changes.
Imaging follows in almost every case. MRI gives physicians a clear view of the discs, nerve roots, and surrounding soft tissue without radiation exposure. It shows whether a disc herniation or narrowing of the spinal canal is pressing on a specific nerve root and at which level.
When the clinical picture is unclear or symptoms have persisted for an extended period, physicians may order electromyography and nerve conduction studies, known as EMG/NCS. These tests measure the electrical activity of muscles and the speed at which nerves conduct signals, confirming which nerve is affected and how significantly.
It's time to get back
to doing what you love.
Treatment: Starting Conservative, Progressing When Needed
The good news is that most patients with lumbar radiculopathy don’t need surgery. Conservative treatment works well for the majority of cases, and that’s always where care begins.
Physical therapy forms the foundation of early treatment. Therapists work to reduce nerve irritation, strengthen the muscles that support the spine, and retrain movement patterns that may be aggravating the affected nerve root. Anti-inflammatory medications help manage pain during the acute phase, and oral steroids are sometimes prescribed for a short period to reduce inflammation more aggressively. For patients whose symptoms are making it difficult to participate in therapy or get through the day, epidural steroid injections can deliver targeted relief directly to the area that needs it.
When conservative care hasn’t produced enough improvement after an adequate time, or when symptoms include significant muscle weakness or signs of progressive nerve involvement, surgery becomes a reasonable next step. The most common procedure for lumbar radiculopathy caused by a herniated disc is a microdiscectomy. It’s a minimally invasive approach that removes the disc material pressing on the nerve root while leaving the surrounding tissue largely undisturbed. Many patients notice relief quickly and return to normal activity within a few weeks.
The decision to move forward with surgery never rests on imaging alone. At Neurosurgeons of New Jersey, the conversation starts with what the patient is actually experiencing, how long they’ve been living with it, and whether prior treatments gave the nerve a fair chance to recover.
When to Schedule an Evaluation
If you’ve been managing leg pain, numbness, or weakness that traces back to your lower back, it’s worth getting evaluated. Seeing a specialist doesn’t mean committing to surgery. It means getting an accurate picture of what’s happening and understanding your options clearly.
A few symptoms call for prompt attention rather than a wait-and-see approach: progressive leg weakness, any changes in bladder or bowel function, or pain severe enough to disrupt your ability to function day to day. These can indicate a level of nerve compression that benefits from faster intervention.
For everything else, the goal is a plan that makes sense for your situation and one you feel confident moving forward with, whether that’s physical therapy, an injection, additional imaging, or a broader conversation about what surgical care would actually involve.
You do not have to figure this out on your own. Our team is here to listen, evaluate what you are experiencing, and help you understand your next steps clearly.
Schedule an evaluation with Neurosurgeons of New Jersey and get answers you can feel confident about.
Frequently Asked Questions
What is the difference between lumbar radiculopathy and sciatica?
Sciatica refers specifically to irritation of the sciatic nerve, which forms from several nerve roots in the lower lumbar and sacral spine. Lumbar radiculopathy is the broader clinical term covering compression or irritation of any lumbar nerve root. Sciatica is one specific type of lumbar radiculopathy.
Can lumbar radiculopathy heal on its own?
In many cases, yes. Disc herniations can shrink over time, and nerve irritation often improves with conservative care. Most patients see meaningful improvement within six to twelve weeks, though the timeline varies depending on the severity of compression and how the body responds.
Is lumbar radiculopathy the same as a pinched nerve?
It’s the clinical term for what most people call a pinched nerve in the lower back. The nerve root faces compression or irritation at the point where it exits the spine.
How long does treatment take?
It depends on the cause, the severity of nerve involvement, and how the patient responds to initial treatment. Some patients improve significantly within a few weeks. Others work through a longer course of conservative care or eventually decide to move forward with a surgical option.
Do I need surgery for lumbar radiculopathy?
Most patients don’t. Conservative treatment, physical therapy, medication, and time resolve the majority of cases. Surgery enters the conversation when those approaches haven’t provided adequate relief or when there are signs of progressive neurological involvement that need a more direct solution.
Dr. Anthony Conte, MD
Dr. David Estin, MD, FACS
Dr. Christopher Gillis, MD, FRCSC, FAANS
Dr. Jonathan H. Lustgarten, MD
Dr. Ty J. Olson, MD, FACS

About Dr. Anthony Conte
Dr Conte is a distinguished graduate of an eight-year combined BA/MD program, receiving his bachelor's degree magna cum laude from Siena College and his Doctor of Medicine from Albany Medical College. During his time in Albany, he was inducted into the prestigious Alpha Omega Alpha Honor Society. He completed his residency training at Georgetown University, where he not only served as Chief Resident but also received extensive training in minimally invasive spine surgery techniques. Following his residency, Dr Conte pursued a subspecialized fellowship in complex and reconstructive spine surgery at Northwestern University.Dr Conte’s medical practice is primarily focused on the treatment of various spinal pathologies using minimally invasive techniques. He is skilled in performing minimally invasive cervical and lumbar fusions through posterior, lateral, and anterior approaches, often utilizing imaging guidance and intraoperative navigation to minimize incisions and reduce surgical time. A strong advocate for cervical and lumbar arthroplasties and disc replacements, he aims to preserve motion in the spine and limit future degeneration. Additionally, Dr Conte specializes in managing complex spine conditions, including revision spine reconstruction surgery, scoliosis, spinal tumors, and spinal vascular lesions. His expertise also extends to treating a variety of brain conditions, such as tumors and hemorrhages.




